Sheath Removal
After the procedure is completed, the patient is taken to the holding area for sheath removal. Removal of the sheath is not without risk and proper precautions should be considered prior to removal. The following baseline information should be reviewed prior to sheath removal:
- Clotting time - Make sure that patient's coagulation (aPTT, PT/INR) status is withing normal range. If patient has recieved anticoagulants, sheath removal should be delayed until clotting time can return to normal. Elevated clotting times can lead to bleeding complications post sheath removal.
- Platelet count - Platelets are responsible for plug formation at the arteriotomy. Platelets can be inhibited by medications such as Aspirin or Plavix.
- Baseline vital signs - Be aware of what the vital signs are before the sheath is removed. A patient with an elevated blood pressure can impede the clotting ability at the puncture site. A change in vital signs can indicate a complication such as vagal episode or internal bleeding.
- Tissue abnormalities - Assess the site for currently abnormalitied that obscure anatomical landmarks. Hematomas can occur during the procudure and can complicate the sheath removal process as well as cause additional pain to the patient. Exisiting hematomas should have the borders outlined so that they can be assessed for growth during the sheath removal
- Functioning IV - If complications occur during sheath removal, then a functioning IV will be essential for medication and fluid administration.
- Patient cooperation - It will be important for the patient to keep the affected extremity imobile during and after sheath removal to prevent clot dislodgement from the puncture site. Knee imobilization may be necessary for the confused and uncooperative patient.
Before you remove the sheath, gather all necessary supplies:
- Sterile 4 x 4's
- Sterile suture removal device
- Clean and sterile gloves
- Personal protective equipment (gown, mask, eyewear)
- Antibiotic ointment
- Sterile dressing
- Atropine 1mg
Prepare the patient for what to expect during the sheath removal. Explain that there will be discomfort during while pressure is applied to the puncture site. Encourage the patient to breathe normally and to not bear down during the sheath removal and while pressure is held. Allow the patient to void in order to avoid a distended bladder. Answer all questions.
The patient should be connected to non-invasive monitoring with the blood pressure cycling every 5 minutes. Vaso-vagal symptoms to observe for include: decreased heart rate, decreased blood pressure, decreased level of consciousness, nausea and vomiting, and cool, clammy skin. Retro-peritoneal bleeding symptoms to observe for include: increased heart rate and decreased blood pressure.
Position the patient for optimal sheath removal. Have the patient in a supine position with the head of the bed flat. Pull the ankle away from midline, about 10 - 12 inches apart from the opposite ankle, so to expose the femoral head for better positioning over the arterial access site. Outward Rotation of the foot helps to move the inguinal ligament away from the femoral artery.
While wearing clean gloves, remove the current dressing and assess the site for presence of hematoma. Open necessary supplies and have them easily accesible. Don personal protective apparel and sterile gloves and remove existing suture around the sheath.
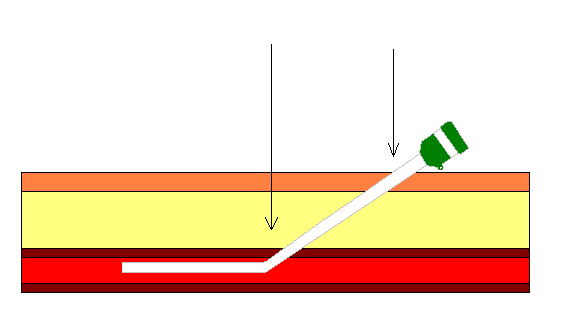
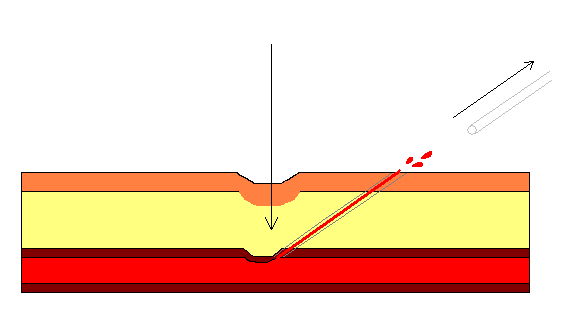
Because the sheath is inserted at a 45 degree angle, the arterial anastomosis is approximately 1/2 inch above the skin insertion. Use your 3 middle fingers to palpate the pulse above the insertion site. Inform the patient that you are about to apply pressure, then remove the sheath while applying gentle pressure without "stripping" clot from the sheath into the artery. Once the sheath is out, allow a spurt of blood to purge the tract of any blood clot then apply firm pressure over the artery.
Manual pressure is held at full pressure for the first 5 minutes then tapered over the next 10 - 15 minutes (per hospital protocol for length of manual pressure) until hemostasis is obtained.
While you are holding pressure with one hand, use the other hand to palpate the surrounding tissue for hematoma formation. If an area is under question, you can always check the other groin for comparison. If a venous sheath needs to be pulled, it should be done 5 minutes after the arterial sheath is pulled in order to decrease the risk of arteriovenous fistula formation.
Once hemostasis is obtained, remove your hand slowly and observe the site for 1 - 2 minutes. If bleeding occurs, continue pressure at the site until hemostasis is achieved. Apply antibacterial ointment to puncture site and cover with a sterile dressing (folded 4 x 4 guaze with Opsite) and give the patient post procedure instructions regarding bedrest (laying flat for 4 - 6 hours with both head and leg, hold mild pressure over bandage if they need to cough or sneeze, ask nursing staff for assistance and notify them if warm bleeding sensation is felt in the groin area).
References
- Baim, D.S. (2005) Grossman's Cardiac Catheterization, Angiography, and Intervention. (7th ed.). Philadelphia,Pa: Lippincott, Williams & Wilkins.
- Kern, M. et al (2003) The Cardiac Catheterization Handbook (4th ed.). Philadelphia, Pa: Mosby.
- O'brien C., Recker, D. How to Remove a Femoral Sheath. AJN. Oct 1992;92(10):34-37.