Percutaneous Coronary Intervention
Percutaneous Coronary Intervention (PCI) includes a variety of techniques aimed at treating ischemic coronary artery disease. Originally termed Percutaneous Transluminal Coronary Angioplasty (PTCA), PCI has evolved to include techniques such as balloon angioplasty, stents, blades, burrs, and aspiration catheters.
Let's break down PCI. Percutaneous refers to access of the inner body by a needle puncture of the skin, instead of an incision approached to expose the inner body. Coronary refers to the arteries that supply the heart with nutrient rich blood. Intervention refers to an action to improve a situation.
History of PCI
PCI was had its origin in the 1960s with dilation techniques by Dr. Dotter and Judkins. This approach was restricted for clinical application with coronary arteries. In the 1970's, Dr. Gruentzig replaced the dilators with an inflatable balloon used to inflate the lesion. The first PTCA of a stenotic coronary artery in a human took place in 1977.
Balloon angioplasty was the only revascularization technique used until atherectomy catheters and stents were introduced in the 1990s. The first stents were metal stents and became known as bare metal stents (BMS). In the early 2000s, stents had evolved to include a medication that eluted off of the metal stent to prevent cellular proliferation that restenosed the artery. Over the years, stents have evolved with a change in metal and designs that improve their deliverability, strength, and success at keeping the artery open.
How does PCI work
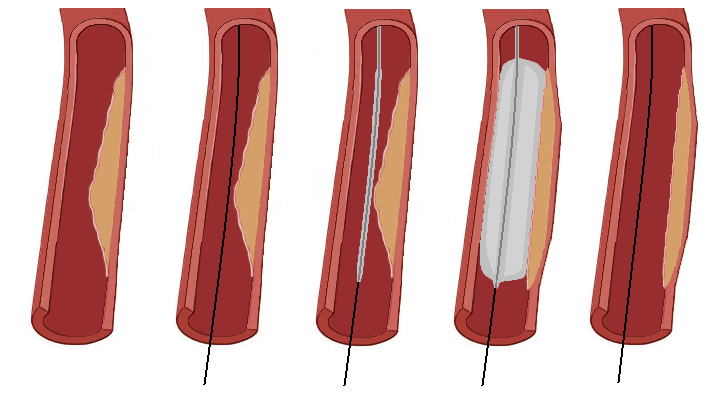
PCI requires a few basic components in order to dilate an artery with a stenotic lesion. The first piece is a guide cathter that allows access, visualizaiton, and delivery of equipment to the artery. The second piece is a guidewire that is advanced across the lesion and allows angioplasty equipment to travel over. The third piece is an interventional catheter (balloon, stent, atherectomy, thrombectomy) that travels to the lesion to revascularize the artery.
The guide catheter is positioned at the ostium of the coronary artery and a thin guidewire is advanced acrossed the lesion into the distal aspect of the artery. The interventional catheter is then advanced by tracking it over the guidewire and positioned at the area of the lesion. Positioned is verified with the injection of contrast media to confirm correct position. The catheter is then inflated to expand the lumenal area of the artery and then deflated to allow blood to resume flow through the artery.
Complications to consider
As the arterial wall becomes compressed by the interventional catheter, small tears and disruptions occur from the shear force of the balloon. This endothelial damage will trigger a healing phase that sends platelets to the site to develop a blood clot. Appropriate anticoagulation therapy will prevent a blood clot from forming that will occlude blood flow at the site of intervention.
After the balloon has been inflated, the inner layer may tear and peel away from the arterial wall. This is known as dissection. If a dissection is headed distally, then it will continue to grow just as wind blows in a sail. Dissection planes will need to be stented to avoid the progression of the disseciton.
Balloon inflation can cause plaque to become dislodged from the arterial wall and embolize down stream potentially occluding a distal branch of the artery. Further intervention may be required to reestablish blood flow to the region.
Abrupt closure of the artery may occur from the elastic recoil nature of the artery. Stretching of the artery with a balloon catheter usually causes the arterial wall to lose its elastic property.
Perfuration of the arterial wall is the most catastrophic complication that can occur with interventional equipment. Immediate treatment is required to prevent blood from flowing into the pericardial space. Balloon inflation to completely occluded the perforated area is usually performed until subsequent therapy can be perfomred. The perforation is usually treated with a covered stent. Pericardiocentesis to drain fluid from the pericardial space is usually performed.
Plaque shifting may occur during inflations. This shifting can cause a narrowing distal to the area treated and may occlude a nearby side branch. If a side branch becomes occluded due to plaque shifting, angiplasty at the region may be required.
References
- Baim, D.S. (2005) Grossman's Cardiac Catheterization, Angiography, and Intervention. (7th ed.). Philadelphia,Pa: Lippincott, Williams & Wilkins.
- Kern, M. et al (2003) The Cardiac Catheterization Handbook (4th ed.). Philadelphia, Pa: Mosby.