Fractional Flow Reserve
Fractional Flow Reserve (FFR) is a measurement of the functional severity of a coronary lesion. During coronary angiography, the severity of a lesion is judged by visual inspection and is considered severe, or flow limiting, if the vessel diameter narrowing is estimated to be 70% or greater. FFR is measured as the ratio of distal blood flow in a vessel with a coronary lesion to the normal blood flow at the proximal region of the vessel. This measurement is obtained during maximum arteriolar vasodilation, also referred to as maximum myocardial hyperemia. FFR contributes to the decision whether a lesion should be treated medically, receive coronary intervention, or revascularization.
How does FFR work?
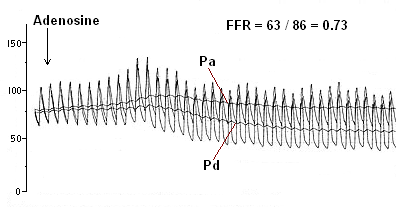
FFR measures the mean arterial pressure in the coronary artery beyond a lesion and divides it by the normal mean arterial pressure proximal to the lesion. The functional state of the lesion is determined by the maximal blood flow that can reach the heart muscle. A state of myocardial hyperemia is induced to determine if the distal blood flow is no longer sufficient to meet the oxygen demand of the heart muscle.
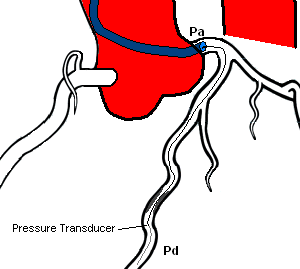
FFR is calculated as Pd / Pa. (Pd = pressure distal to the lesion, Pa = pressure proximal to the lesion) The mean pressure measured by the pressure wire is divided by the mean pressure measured by the catheter.
FFR results
FFR results can be interpreted as:
- FFR 1.0 = normal blood flow
- FFR > 0.80 = ischemia is very unlikely
- FFR < 0.75 = specific indication for ischemia
How is FFR performed?
FFR is performed very much like an interventional procedure. The patient is given anticoagulation medication to prevent blood clot formation on the wire while it remains in the coronary artery. Appropriate size catheters are chosen for optimal hemodynamic monitoring for FFR. This is usually performed using 6 FR sheath and guide catheters, but can be used in a 5 FR system.
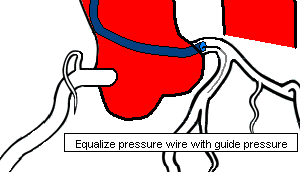
The FFR wire, a 0.014" wire with a pressure transducer near the tip, is zeroed and then advanced through the catheter to the ostium of the coronary artery. The wire pressure must then be equalized with the catheter pressure. The wire is then advanced into the coronary artery past the lesion. Once the transducer of the pressure wire is positioned beyond the lesion, baseline FFR is calculated. If the baseline FFR is greater than 0.75, then a hyperemic agent is administered (Adenosine) and FFR is calculated.
Adenosine Administration
Adenosine can be administered Intra-coronary (IC) or Intra-venous (IV) to induce maximum myocardial hyperemia. Intra-coronary injections are usually performed while Intra-venous infusions are used with ostial lesions of the Left Main or Right Coronary Artery.
Adenosine induces maximum hyperemia by causing endothelial relaxation of smooth muscle found inside the arterial wall. This causes dilation of the arteries and results in an increase of blood flow to the myocardium of the heart. An artery with a lesion will not allow the increased demand of blood flow to the distal myocardium.
To acheive maximum hyperemia, Adenosine is usually given in bolus doses of 15 - 30 mcg for the right coronary artery and 20 - 40 mcg for the left coronary artery. Intra-venous infusions of Adenosine is given in a dose of 140 mcg/kg/min over 3 - 4 minutes. The Intra-venous infusion has been the gold standard of administration in order to acheive maximum hyperemia, but is also associated with more systemic adverse effects. Some clinicians have begun to use even higher doses of IC Adenosine for maximum hyperemia in order to acheive the same effect that Intra-venous infusion delivers. There is data to support this practice, but it is also viewed that those who give higher doses are non-believers and only want to treat the lesion in hopes of lowering the FFR.
Remember that Adenosine is used as a rapid bolus to treat supraventricular tachycardia (SVT) by inducing heart block at the AV node. Careful consideration should be used with Intra-coronary doses for the right coronary artery. Asytole may be noted with higher doses injected into the right coronary with a return to the patient's baseline rhythm.
References
- Pijls NH, Fearon WF, Tonino PA, Siebert U, Ikeno F, et al. Fractional Flow Reserve Versus Angiography for Guiding Percutaneous Coronary Intervention in Patients With Multivessel Coronary Artery Disease. 2-year follow-up of the FAME (Fractional Flow REserve Versus Angiography for Multivessel Evaluation) Study. J Am Coll Cardiol. 2010;56(3):177-184.
- Pijls NH, De Bruyne B, Peels K, Van Der Voort PH, Bonnier HJ, Bartunek J Koolen JJ, et al. Measurement of Fractional Flow Reserve to Assess the Functional Severity of Coronary-Artery Stenosis. N Engl J Med 1996; 334:1703-1708
- Tonino PA, De Bruyne B, Pijls NH, Siebert U, Ikeno F, van't Veer M, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. Jan 15 2009;360(3):213-24.